Interesting Case of the Month - (IGHP, ICOM) - November
november 2025
Clinical History-
43-year-old femalewith h/o lump in left upper abdomen with off and on pain, H/o upper GI bleed-3 episodes in last 1 year requiring blood transfusion and EVL. No H/o jaundice, ascites hepatic encephalopathy, LFT’s Bili-1.6/ 0.3, SGOT/ SGPT-35/ 43, ALP/ GGT 57/ 18, Albumin 3.9, PT/ INR-15.2/ 1.3. Viral markers HBsAg and Anti HCV non-reactive.
From the images below identify the likely disease?
Radiology-
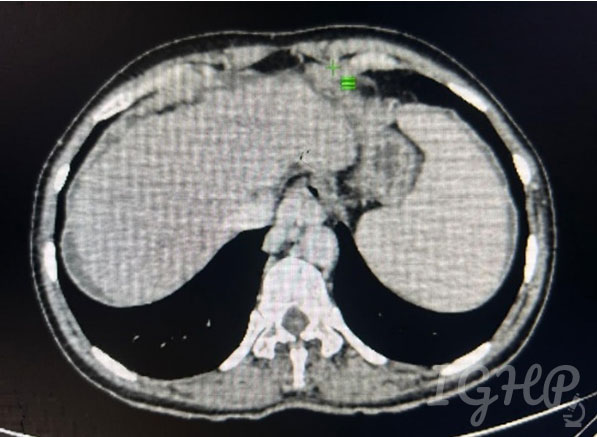
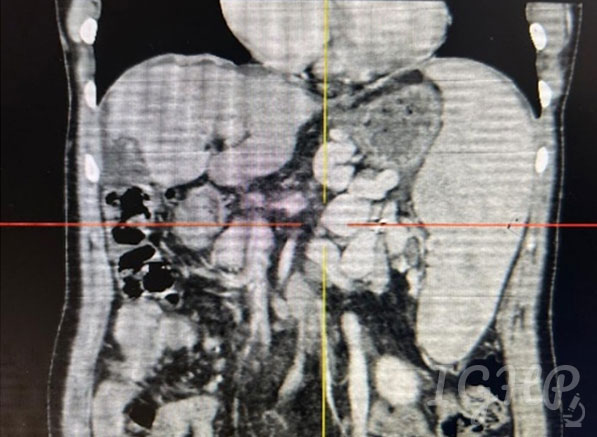
CECT Abdomen-
Cirrhotic liver with splenomegaly with dilated splenic vein and multiple dilated torturous collaterals in peripancreatic splenic hilar peri gastric and lienorenal region. Portal vein 10mm, No ascites.
Fibro scan 12.6 Kpa
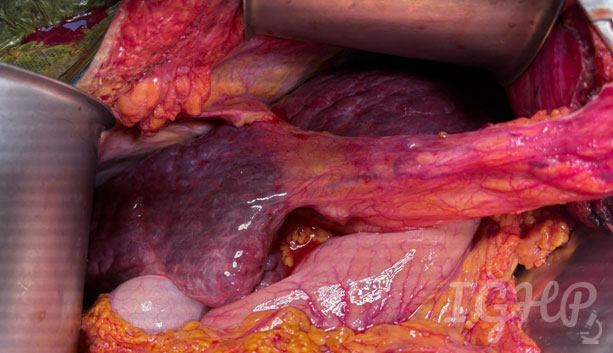
Intraoperative Image-
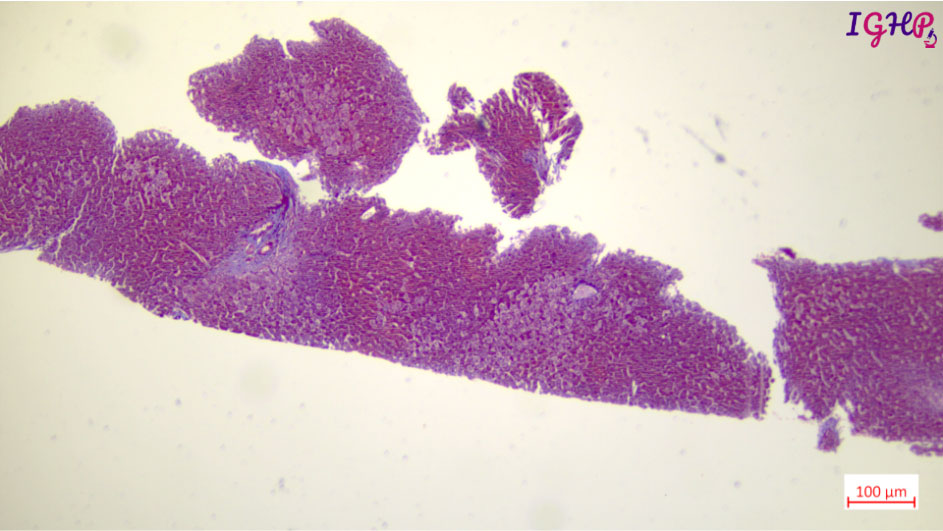
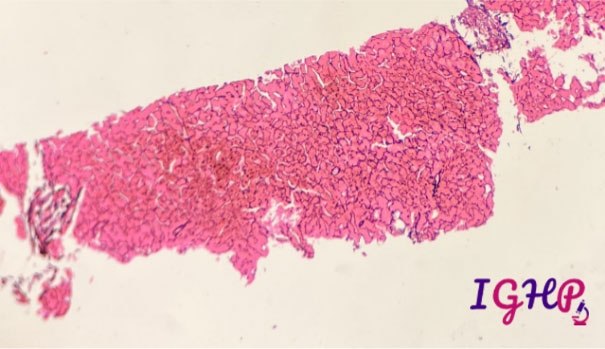
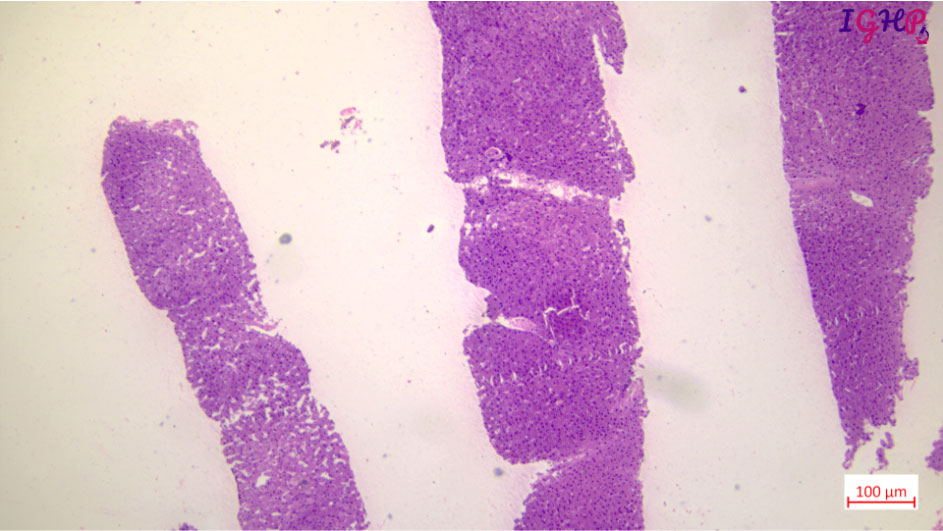
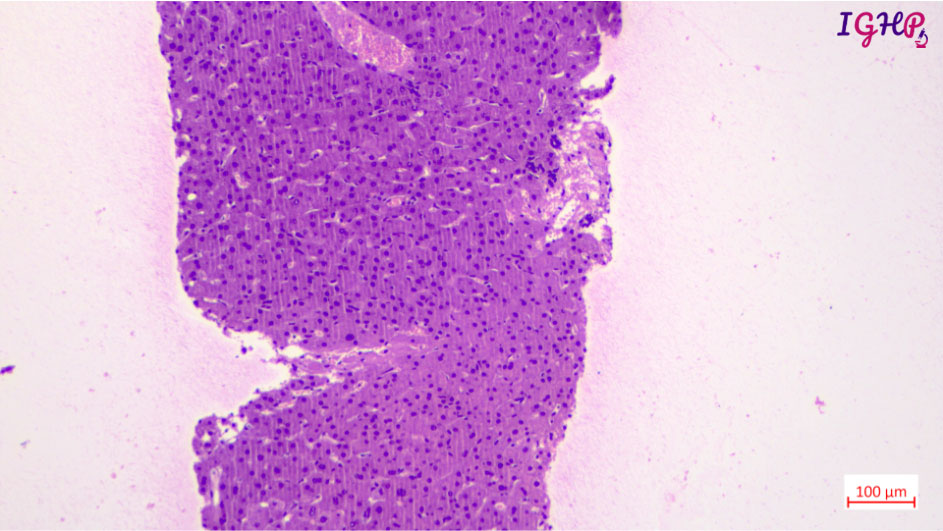
Microscopic Images-
Microscopic examination showed variable distortion of liver architecture with irregular distribution of portal tracts. At places the tracts appear atrophic with areas of close approximation. Few tracts showed absence of portal venous profiles and hypertrophied arterial vessels. There is presence of thin delicate blind ended fibrous septae around few of the portal tracts.
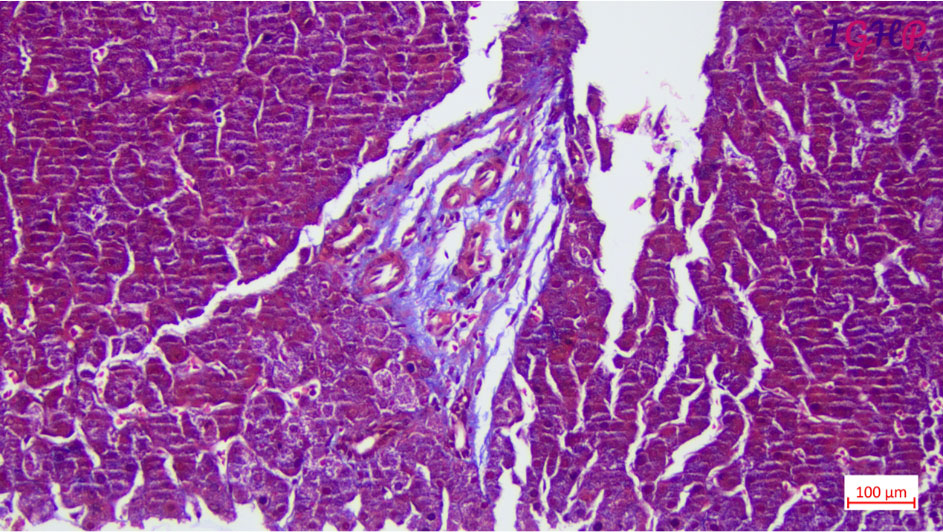
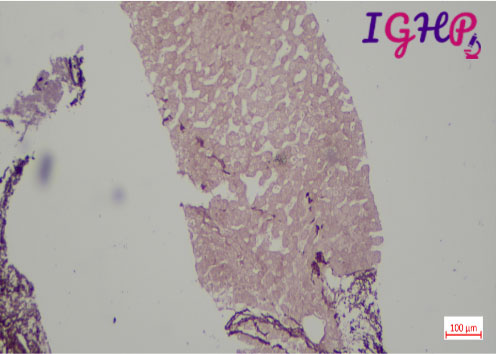
Special Stain Performed-
MT, Orcein and Reticulin stains performed showed maintained liver cell plate network with presence of thin delicate blind ended septae around few of the portal tracts.